Adenosine is a naturally occurring purine nucleoside that forms from the breakdown of ATP (adenosine triphosphate). ATP is the primary energy source in cells for transport systems and many enzymes. Adenosine facilitates tumor survival by a variety of mechanisms. Adenosine can bind to purinergic receptors in different cell types where it can produce a number of different physiological actions. Adenosine accumulates in solid tumors and stimulates tumor growth and tumor angiogenesis while imparting tumor resistance to the immune system.
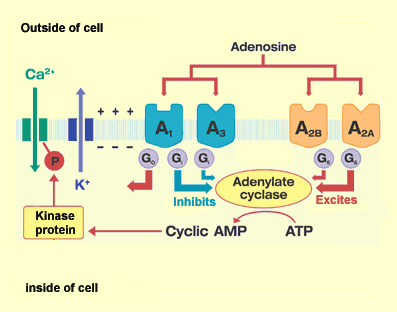
Extracellular adenosine initiates most of its effects through the activation of adenosine receptors. There are at least four subtypes of the adenosine receptor A1, A2A, A2B and A3 receptors. Adenosine receptors are all coupled to G-proteins and the A1 and A3 subtypes are associated with inhibitory G-proteins. Each of these four cell surface adenosine receptors (ARs) is found to be upregulated in various tumor cells. It is overexpressed in inflammatory and cancer cells, while low expression is found in normal cells. The adenosine receptors are important and ubiquitous mediators of cellular signaling, which play vital roles in protecting tissues and organs from damage. In particular, adenosine triggers tissue protection and repair by different receptor-mediated mechanisms, including an increase of oxygen supply/demand ratio, preconditioning, anti-inflammatory effects, and stimulation of angiogenesis. Activation of the receptors by specific ligands, agonists or antagonists, modulates tumor growth via a range of signaling pathways. At the present time, it can be speculated that adenosine A1, A2A, A2B, and A3 receptor-selective ligands may show utility in the treatment of cancer and other disorders in which inflammation is a feature.
Introduction to adenosine receptors as therapeutic targets.
Adenosine receptors and cancer.
Enhancement of tumor immunotherapy by deletion of the A(2A) adenosine receptor.
A3 adenosine receptor as a target for cancer therapy.
The A3 adenosine receptor as a new target for cancer therapy and chemoprotection.
Adenosine A2B Receptor Blockade Slows Growth of Bladder and Breast Tumors.
Hypoxia-inducible adenosine A2B receptor modulates proliferation of colon carcinoma cells.
Methylxanthines, such as caffeine and theophylline, can function as antagonists of adenosine receptors, and their stimulant actions occur primarily through this mechanism. Theophylline is a prescription medication to treat airway spasms in people with asthma or COPD. Caffeine is a mild stimulant. It can be found in many weight loss pills to boost the metabolism. But there are a number of additional situations where caffeine can serve important medical uses. Several studies have found connections between caffeine and cancer. Caffeine is similar in structure to adenosine, and binds to those receptors so that adenosine cannot bind. Caffeine acts mainly via blockade of adenosine receptors. In conclusion, targeting approaches that involve ARs will enhance the possibilities to cure cancer naturally, via the universally consumed substance that is caffeine.

Emerging adenosine receptor agonists – an update.
Methylxanthines, inflammation, and cancer: fundamental mechanisms.
Xanthines as adenosine receptor antagonists.
Caffeine intake induces an alteration in human neutrophil A2A adenosine receptors.
 Caffeine is a very common substance that is contained in coffee, tea, chocolate, soft drinks, and can also be purchased as capsules, tablets, or powder. An estimated 80% of the world’s population consumes a caffeine-containing substance daily. A typical 8-ounce (240-ml) cup of instant coffee contains about 100 mg of caffeine — about twice as much as a cup of tea or a 12-ounce (360-ml) can/bottle of soda. A 30-gram chocolate bar might contain as much caffeine as half a cup of tea. Pure caffeine can be obtained in powders, caplets or tablets in products like NoDoz, Stay Awake and Vivarin.
Caffeine is a very common substance that is contained in coffee, tea, chocolate, soft drinks, and can also be purchased as capsules, tablets, or powder. An estimated 80% of the world’s population consumes a caffeine-containing substance daily. A typical 8-ounce (240-ml) cup of instant coffee contains about 100 mg of caffeine — about twice as much as a cup of tea or a 12-ounce (360-ml) can/bottle of soda. A 30-gram chocolate bar might contain as much caffeine as half a cup of tea. Pure caffeine can be obtained in powders, caplets or tablets in products like NoDoz, Stay Awake and Vivarin.
It’s generally agreed that consuming up to 300 mg of caffeine per day is safe. That’s roughly the amount of caffeine you would get from three cups (not mugs or big paper cups) of coffee. Consuming more than 300 mg caffeine per day may give you the “caffeine jitters.” Larger amounts of caffeine may make you irritable, sleepless and may even trigger anxiety and cause diarrhea. Some people are more sensitive to caffeine than are others. So we cannot suggest a universally safe dose. However, it is believed that the expected treatment effect of caffeine is time-dependent and dose-dependent. Some packages will use an age range to figure dose, but it is more effective to dose by weight. So, we recommend you take 4.5 mg per pound of body weight (for metric users, that’s 10mg per kilo). For example: a 133-pound woman would get about 600mg (133 X 4.5 =598) caffeine per day (200mg 3times daily) in combination with 5-LOX inhibitor such as BosturZym. BosturZym has synergistic effect with caffeine against cancer and leukemia. You can take them all together.
Lethal Enzyme 5-LOX and Cancer
Please Note: Caffeine in concentrated forms such as pills or powders can accidentally be taken insufficient quantities to cause nausea, vomiting, stomach upset, trouble sleeping, increased urination, or unconsciousness. If any of these effects persist or worsen, tell your doctor or pharmacist promptly. A single box of Vivarin or No-Doze can be fatal if taken at one time. Although possible with coffee or other strongly caffeinated drink, it generally requires much more awareness of the large dosage before dangerous levels are reached.
Oral Caffeine Dosages
Onset : 5 – 10 minutes
Duration : 1.5 – 5 hours, Normal After Effects : up to 24 hours



{kind=link}