 Throughout the years, there has been research on the negative and positive effects of marijuana on the human body and the brain. Marijuana is frequently beneficial to the treatment of AIDS, cancer, glaucoma, multiple sclerosis, and chronic pain. Marijuana plant contains 400 chemicals and 60 of them are cannabinoids, which are psychoactive compounds that are produced inside the body after cannabis is metabolized or is extorted from the cannabis plant.
Throughout the years, there has been research on the negative and positive effects of marijuana on the human body and the brain. Marijuana is frequently beneficial to the treatment of AIDS, cancer, glaucoma, multiple sclerosis, and chronic pain. Marijuana plant contains 400 chemicals and 60 of them are cannabinoids, which are psychoactive compounds that are produced inside the body after cannabis is metabolized or is extorted from the cannabis plant.
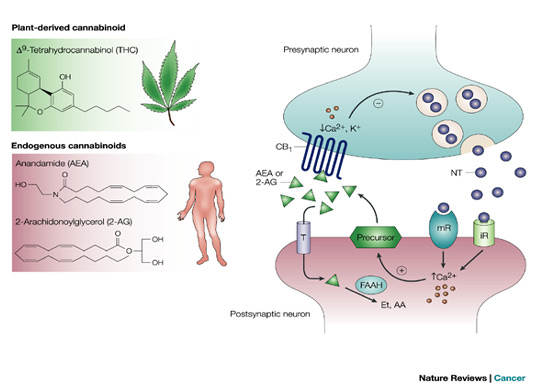
Cannabinoids is an active ingredient of marijuana. The most psychoactive cannabinoids chemical in marijuana that has the biggest impact on the brain is tetrahydrocannibol, or THC. THC is the main active ingredient in marijuana because it affects the brain by binding to and activating specific receptors, known as cannabinoid receptors. “These receptors control memory, thought, concentration, time and depth, and coordinated movement. THC also affects the production, release or re-uptake (a regulating mechanism) of various neurotransmitters.” Neurotransmitters are chemical messenger molecules that carry signals between neurons. Some of these affects are personality disturbances, depression and chronic anxiety.

At present, the term “medical marijuana” refers to its use as a pain killer and as a treatment for chemotherapy induced nausea and vomiting. Although these are commendable properties of marijuana, the scientific literature is clear that the major medical benefits of marijuana derived chemicals are their impressive capacity to kill a wide diversity of cancer cells. One of the major medical uses for THC is in the treatment of glioma or brain cancer. THC enters the brain, which is rather obvious. THC is very toxic to glioma cells but not their normal counterpart, astrocytes. In fact, THC protects astrocytes from oxidative stress. Since there are very few treatments for brain cancer, the use of THC in the treatment of brain cancer should be seriously explored.
THC activates the ceramide, or death pathway in the brain and this kills cancer cells without inflammation. All cancers need VEGF to stimulate new blood vessel growth into tumors. THC blocks the VEGF pathway effectively in the brain. Keep in mind that Avastin, the Genentech monoclonal antibody that blocks the VEGF receptor, is useless for lesions in the brain. Monoclonal antibodies do NOT enter the brain unless the blood brain barrier(BBB) is incredibly damaged. THC kill a diversity of cancer cells including brain cancer (glioma, glioblastoma), lung cancer, thyroid cancer, skin cancer, breast cancer, uterine cancer, prostate cancer, neuroblastoma, pancreatic cancer, colorectal cancer, lymphoma, leukemia and melanoma.
In addition, THC inhibits the expression of the membrane protein p-glycoprotein. This famous protein is partially responsible for the resistance to a host of different chemo drugs. As soon as the drugs enter the cancer cells, p-glycoprotein pumps them out again. Therefore, THC both reduces the nausea associated with chemotherapy AND blocks the multidrug resistance (MDR) associated with the use of these drugs. In simple terms, THC improves the clinical efficacy of these drugs.
THC binds the CB1 and CB2 receptors, which are activated by endogenous compounds (endocannabinoids) and are involved in a wide range of physiopathological processes (e.g. modulation of neurotransmitter release, regulation of pain perception, and of cardiovascular, gastrointestinal and liver functions). The activation of the CB1 receptor is largely associated with the alleviation of pain. The CB2 receptor has been less extensively studied. Current research links the activation of the CB2 receptor to programmed cell death in cancer cells, and the maintenance of bone mass. The activation of the CB2 receptor activates the ceramide death pathway, one of the most powerful apoptosis or programmed cell death pathways known. Ceramide stimulates the upregulation of the p8 stress regulated protein. This protein upregulates a host of different endoplasmic reticulum stress related genes including ATF-4, CHOP and TRB3. The protein produdcts of these genes induces apoptosis in cancer cells.
In addition to its specific ability to activate the CB1 and CB2 receptors, THC can diffuse into CB1/2 negative cells and destabilize mitochondrial functioning. This leads to programmed cell death. This is particularly prominent in cancer cells. Normal cells, including neurons and astrocytes, are actually protected against death by THC. THC downregulates ERK and PI3K/AKT cellular signaling. The AKT enzyme is a critical survival factor for all cancer and leukemia cells. It must be inhibited at all costs.
THC activates various receptors which induce cell death by activating the ceramide death pathway. It probably wouldn’t take too much THC to kill these cells. The problem is that the THC metabolites activate more than one membrane receptor in brain cells. Some receptors activate psychotropic or pleasure responses while others activate death pathways in the cancer cells. The effects of THC on brain and other cancer cells are well documented in the scientific literature. It kills them!! THC metabolites also kill breast cancer, skin cancer and leukemia cells, but destroying brain cancer cells is the big deal. The reasons are simple. It is very difficult to get active chemotherapy chemicals into the brain to destroy brain cancer cells. THC metabolites enter the brain readily. In the US, this type of treatment would not be permitted. In the interim, if you have brain cancer or metastasis to the brain, consider getting treated in Canada.
When taken orally, cannabinoids are not very well absorbed and often have unpredictable effects. Patients often become sedated or have intoxication-like symptoms when THC is metabolized by the liver. A small number of studies with Marinol (synthetic THC in sesame oil in a gelatin capsule) and Cesamet (synthetic THC analogue) have shown some effectiveness in pain relief, but optimal doses that relieve pain often cannot be achieved because of unpleasant psychologic side effects.
Inhaling cannabinoids, especially THC, also may cause problems for many patients. Blood levels rise suddenly and then drop off sharply. This rapid on-off effect may produce significant intoxication, particularly in patients who are new to cannabinoids. This may pose the risk of abuse potential. Smoking cannabis produces this effect, which is the very reason that recreational users prefer the inhaled route. Patients, however, generally wish to avoid psychologic effects, and it is unclear how difficult it might be to find a dosing pattern that enables them to have pain control without side effects.
Sativex was approved by Health Canada in June 2005 for marketing as an adjunctive medicine for central neuropathic pain in multiple sclerosis. Adjunctive therapy means taking two or more medications to help control pain. Sativex has a different delivery system – an oromucosal/sublingual spray absorbed by the lining of the mouth – that, according to the manufacturer, generally allows patients to gradually work up to a stable dose at which they obtain therapeutic pain relief without unwanted psychologic effects. These synthetic THC have shown therapeutic effects in patients with brain cancer. Synthetic THC is similar to THC but not the same, which gives less psychoactive effects.
References
1. Non-psychotropic plant cannabinoids: new therapeutic opportunities from an ancient herb.
2. Phytocannabinoids and endocannabinoids.
3. Naturally occurring and related synthetic cannabinoids and their potential therapeutic applications.
4. Cannabinoids in the treatment of cancer.
9. The multidrug transporter ABCG2 (BCRP) is inhibited by plant-derived cannabinoids.
11. Cannabinoids mediate analgesia largely via peripheral type 1 cannabinoid receptors in nociceptors.
12. A house divided: ceramide, sphingosine, and sphingosine-1-phosphate in programmed cell death.
13. Cannabinoid receptors as novel targets for the treatment of melanoma.
14. Recent advances in the immunobiology of ceramide.
17. The stress-regulated protein p8 mediates cannabinoid-induced apoptosis of tumor cells.
18. The effects of cannabinoids on P-glycoprotein transport and expression in multidrug resistant cells.
19. Characterization of P-glycoprotein inhibition by major cannabinoids from marijuana.
20. Peripheral cannabinoid receptor, CB2, regulates bone mass.
21. Cannabinoid receptor ligands mediate growth inhibition and cell death in mantle cell lymphoma.
22. Cannabis and tobacco smoke are not equally carcinogenic.
23. p38 MAPK is involved in CB2 receptor-induced apoptosis of human leukaemia cells.
25. Cannabinoids inhibit the vascular endothelial growth factor pathway in gliomas.
26. Hypothesis: cannabinoid therapy for the treatment of gliomas?
27. Cannabinoids: potential anticancer agents.
28. Inhibition of tumor angiogenesis by cannabinoids.
29. Inhibition of skin tumor growth and angiogenesis in vivo by activation of cannabinoid receptors.
30. Targeting CB2 cannabinoid receptors as a novel therapy to treat malignant lymphoblastic disease.


{kind=link}
{kind=link}